Your periods are heavy if you are changing pads too often, requiring large pads, needing to change at night time, flooding and passing clots. You might feel exhausted and lack of energy. Common causes are fibroids, polyps and thickening of the inner lining of the uterus.
If your periods are not only heavy but also severely painful as well, then adenomyosis (pronounced as aden-no-my-osis) might just be the underlying culprit.
If you have not heard about adenomyosis, you are not the only one. Adenomyosis is a little known and under recognised condition that can cause heavy and painful periods. You might have had an ultrasound but told that your uterus is normal and just some fibroids. Adenomyosis can have rather subtle appearance on ultrasound and be easily missed. You might have been put on hormone pills or a Mirena IUD. If these treatments are not working, you might have been told to put up with the symptoms or have a hysterectomy.
Read on to learn more about adenomyosis, its diagnosis and treatments, and how to avoid a hysterectomy.
What is uterine adenomyosis?
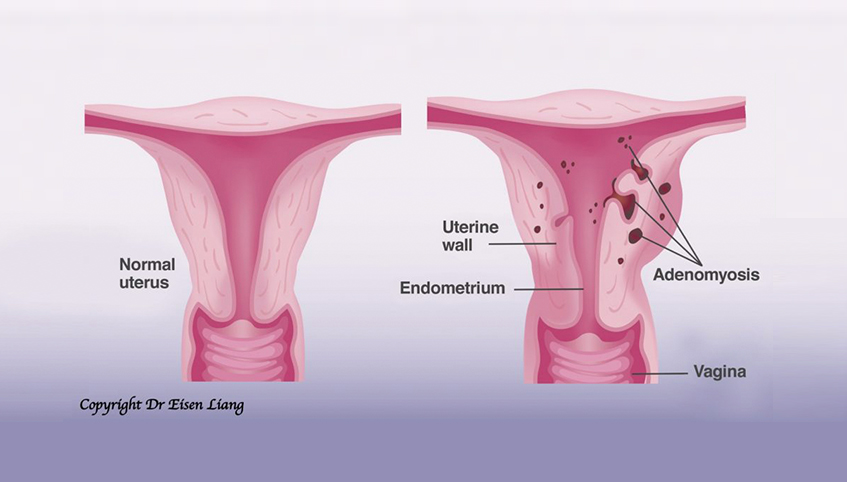
Adenomyosis is like endometriosis within the uterine muscle wall. Adeno (glands) has grown into the uterine muscle wall (myosis). Women with adenomyosis suffers from heavy menstrual bleeding (HMB), in addition to severe period pain. The uterus can be bulky due to reactive thickening of the muscle cells.
Adenomyosis can be found in up to 70% of hysterectomy specimens, and therefore may be far more common than appreciated clinically.
What are the causes of adenomyosis?
We don’t really completely understand what causes adenomyosis. However, there is the suggestion that previous uterine trauma of any kind can lead to development of adenomyosis. The risk factors are multiple pregnancies, termination of pregnancy, uterine curettage and caesarean section.
Adenomyosis is an oestrogen dependent condition and therefore women’s age, early on-set of menstruation, short menstrual cycles, obesity and Tamoxifen use are also risk factors. There is also association between adenomyosis, depression and use of antidepressant medications.
How is adenomyosis diagnosed?
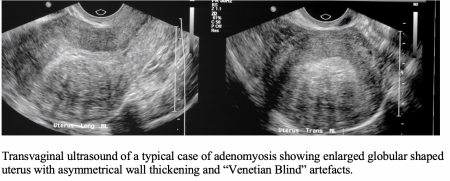
Women’s awareness and clinical suspicion by GPs are the keys to reaching an early diagnosis. Women with adenomyosis typically complain of heavy bleeding and severe period pain. The uterus can be enlarged and tender to touch. Ultrasound can show features of adenomyosis but the signs can be quite subtle and therefore the diagnosis may not be definitive. MRI is more accurate than ultrasound for the diagnosis of adenomyosis, especially if fibroids are also present.
What are the simple measures to treat heavy painful periods?
Non-steriodal anti-inflammatory drugs like Nurofen and Ponstan can ease period pain and lighten heavy bleeding. Tranexamic acid (Cyclokapron) can enhance clotting and reduce heavy bleeding. Contraceptive hormone pills can be taken continuously to avoid having a period. These however might not be the long-term solutions that you are looking for.
How good is Mirena IUD for adenomyosis?

Mirena slowly releases tiny does of progestogen (a sex hormone) over 5 years. Studies have shown that it is effective for relieving the symptoms of heavy bleeding and period pain.
Patient satisfaction rate is 56.3% at 12 months. Common side effects such as prolonged light bleeding (25%) or irregular bleeding (14%), and other less common side effects such as weight gain, ovarian cyst formation, lower abdominal pain and acne contributed to the less than ideal satisfaction rate. Some women also report mood changes with Mirena.
More recent studies have shown Mirena is less effective in women with more extensive adenomyosis, if the uterus is larger than 150ml. A discontinuation rate of 70% is noted in women if the uterus is larger than 314ml.
What is UAE? How does UAE work?
Uterine Artery Embolisation (UAE) is a radiology procedure. It is non-surgical and non-hormonal. UAE is performed under local anaesthetic and light sedation. It requires usually only a 1-night hospital stay and 1-week recovery.
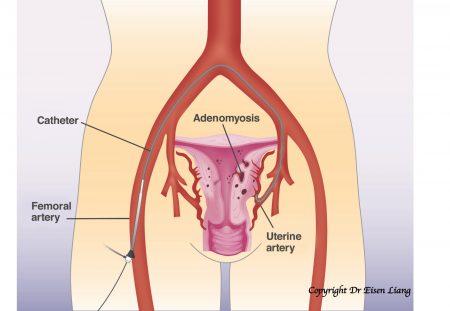
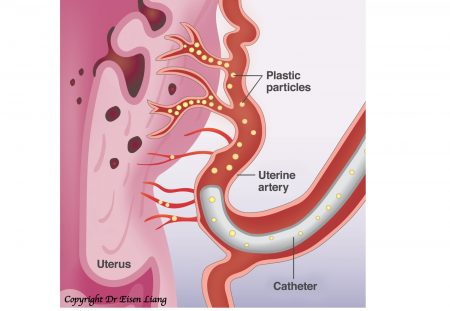
During UAE, a small tube (called catheter) is navigated under X-ray find the uterine arteries. Small particles are injected into the uterine arteries to block the blood supply. The adenomyotic tissue will die due to the lack of oxygen. Normal uterine muscle wall can open up collaterals and therefore isn’t harmed.
Watch the video: “How does UAE work for adenomyosis”
How safe and effective is UAE?
UAE is the probably the most effective non-surgical treatment for adenomyosis. Sydney Fibroid Clinic’s own patient satisfaction rate is 90% – meaning 90% of women treated were happy or very happy with the outcome of their UAE in relieving heavy menstrual bleeding and period pain. There were no major complications.
Case Study:
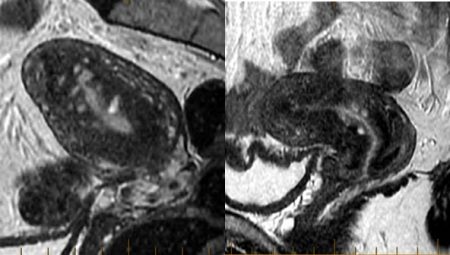
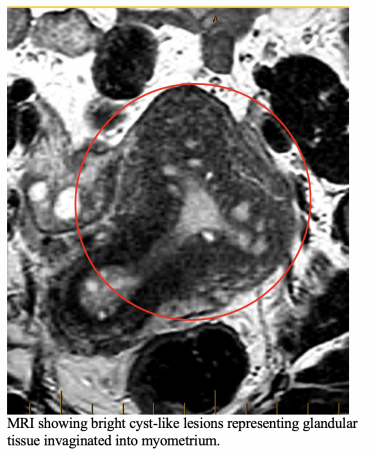
46-year-old hair saloon manager has been suffering from HMB and severe period pain for 10 year. She failed Mirena due to prolonged bleeding and spotting. MRI showed diffuse adenomyosis with large cyst-like bright foci representing glands in the muscle layer that disappeared after UAE. She had a successful clinical outcome with resolution of her HMB and pain. She said her UAE was “liberating”.
Watch video: Elizabeth’s Life-Changing Story about her Adenomyosis and UAE
Is hysterectomy still “the only solution” in the 21st Century?
In the past, hysterectomy was seen as the only definitive treatment for women suffering from adenomyosis related symptoms. From early 2000, reports have emerged documenting the effectiveness of uterine artery embolisation (UAE) as an effective non-surgical alternative to hysterectomy.
Summary
Adenomyosis can cause heavy painful periods. It is often underdiagnosed due to lack of awareness. Ultrasound features are subtle, and MRI may be required to confirm diagnosis. UAE is an effective treatment options for women who prefer to avoid hysterectomies.
Key Points:
- Adenomyosis is like endometriosis within the uterus.
- It can cause debilitating heavy menstrual bleeding and period pain.
- Adenomyosis is often missed by ultrasound; MRI is more accurate.
- Heightened awareness and suspicion are crucial to early diagnosis.
- Hysterectomy is no longer the only solution.
- Uterine Artery Embolization is an effective non-surgical alternative
Dr Eisen Liang is an Interventional Radiologist who founded Sydney Fibroid Clinic. He has worked collaboratively with gynaecologists for more than 10 years in helping women to resolve fibroid related symptoms. His research papers on fibroid disease have been presented internationally and published in ANZJOG.
For further information, please visit www.sydneyfibroidclinic.com.au
