Pelvic Congestion Syndrome Treatment
If you’re experiencing pelvic pain and require treatment, you may have pelvic congestion syndrome. Sydney Fibroid Clinic offers ovarian vein embolisation to treat symptoms of pelvic congestion syndrome.
-
Ovarian Vein Embolisation for Pelvic Congestion
Venous Embolisation is the treatment of choice for Pelvic Congestion Syndrome.
The treatment targets the root cause of pelvic venous congestion: refluxing veins. The embolisation procedure blocks the refluxing veins to stop unnecessary venous backflow into the pelvis, thereby relieving the symptoms caused by congestion. A refluxing vein is a useless vein, overwhelming the exisiting drainage pathways, and therefore can be blocked. Just like how leg varisose veins can be treated by stripping, lasering or injection-to get rid of thse useless veins. Inside the body, we will need to be more gentle, not to harm the adjacent organis like the bowel. Embolisation (blocking) is achieved with soft platimum coils- a very gentle way to treat PCS.
The procedure and its benefits can be summarised as follows:
- Local anaesthetic procedure
- Minimally invasive, safe and effective
- 89% immediate relief and 84% long-term relief (patient satisfaction rates)
- No surgical cuts, no general anaesthetic
- No down time, back to normal activities next day
The local anesthetic procedure is performed by an interventional radiologist in an angiography suite, as a day procedure. A light sedation is given, and the skin entry site is numbed with local anaesthetic. Note: now a days, jugular vein is used for entry into the venous system, and this allows safe access to check and treat all 4 sets of potentially refluxing veins: the left and right ovarian veins, the left and right internal iliac veins.
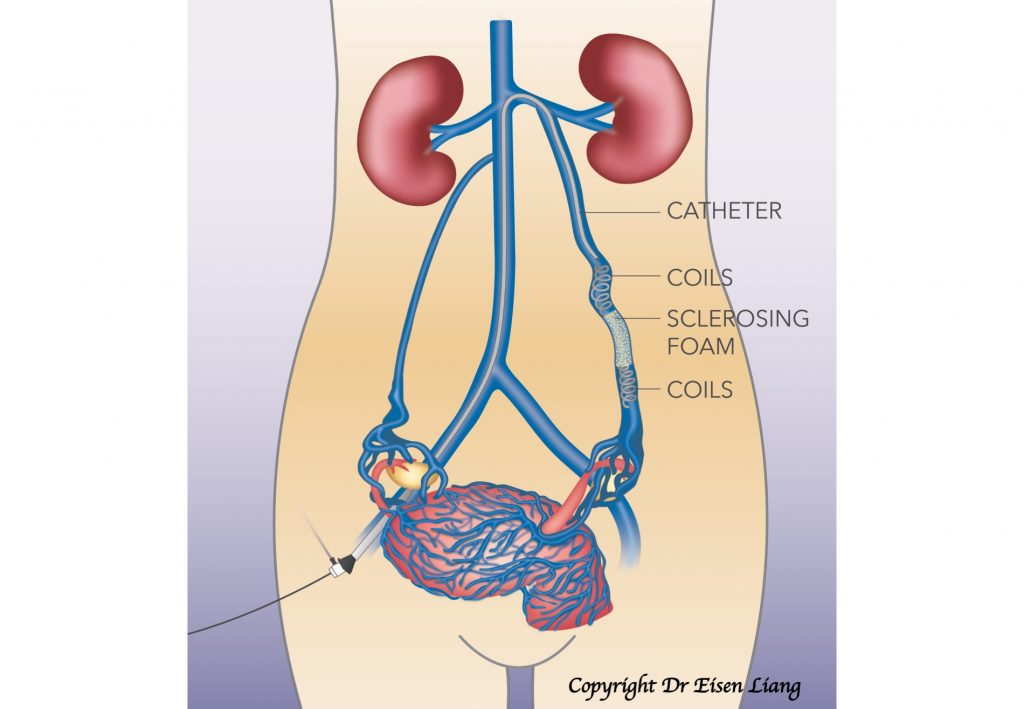
During the process, a tiny nick is made in the skin for a catheter (a small plastic tube) to be inserted. The catheter is navigated inside the vein under X-ray guidance. A diagnostic venogram is performed by injecting X-ray dye to show the veins and direction of blood flow. Once reflux is confirmed, platinum coils are fed through the catheter to the block the vein. A sclerosing agent is injected to secure long-term blockage of the refluxing veins.
The procedure takes about an hour, but it can be longer if additional refluxing veins are found and need to be treated.
Post-procedure, patients require bed rest for 1 – 2 hours until the sedation wears off and will need to arrange transport, as driving is not allowed for 24 hours after sedation. Patients should take it easy at home, drink plenty of fluid and can resume normal activities the following day – though strenuous exercise should be avoided initially. The dressing should be kept in place for two days and then removed. Some patients may experience back and pelvic pain for 1 – 2 days after embolisation, though this can be controlled with Panadol and Nurofen.
For more information on OVE as a pelvic congestion syndrome treatment, make an enquiry with Sydney Fibroid Clinic.
-
Laparoscopic Ligation for Pelvic Congestion
Laparoscopic ligation is a surgical procedure in which a woman’s ovarian veins are tied off. Though tying off the ovarian vein is effective in 80% of patients with pelvic congestion syndrome, it is a much more difficult and invasive procedure than ovarian vein embolisation. The refluxing internal iliac veins cannot be identified or treated by this method. During venous embolisation procedure, all potential refluxing pathways can be tested and blocked if found. Therefore this surgical procedure is not as effective as Venous Embolisation (OVE) and therefore it is rarely performed
-
Hysterectomy for Pelvic Congestion
It is important to note that pelvic congestion syndrome is a venous problem and not a problem of the uterus. Therefore, it does not make sense to remove the uterus.
A hysterectomy for pelvic congestion syndrome is ineffective in a large percentage of patients. Immediately following hysterectomy, pain is still present in in 33% of patients. Recurrence of pelvic pain is noted in 20% of patients. A hysterectomy therefore should not be a treatment for pelvic congestion syndrome.
The cause of pelvic congestion syndrome is the refluxing ovarian vein, which can be effectively blocked non-surgically by ovarian vein embolisation.
Do I Need Treatment?
If pelvic congestion syndrome symptoms are impacting your quality of life, you may need to seek treatment.
If you’re longing for effective pelvic pain treatment and simple measures have not been effective, OVE could be a minimally invasive treatment for you.
If you would like a specialist opinion, get a referral from your GP and book a consultation with Dr Liang.