Pelvic Congestion FAQs
To offer greater insight into pelvic congestion syndrome, pelvic congestion syndrome treatment and ovarian vein embolisation, Sydney Fibroid Clinic has compiled our frequently asked questions.
FAQs about Pelvic Congestion Syndrome (PCS)
-
What causes pelvic congestion syndrome?
Pelvic congestion syndrome is a chronic pain syndrome caused due to distention and congestion of pelvic veins. The root cause is usually reflux in the ovarian vein, allowing backflow of venous blood into pelvis.
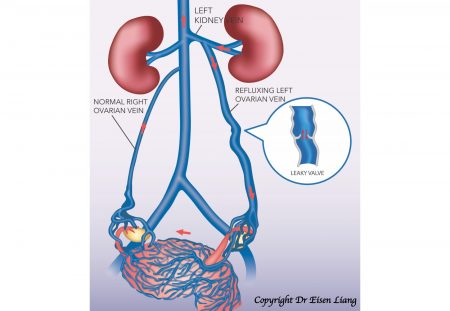
Normal venous valves ensure blood returns towards the heart in one direction, but defective or absent valves cause reflux – blood flow in the reverse direction. Reflux in the ovarian vein creates congestion and raised venous pressure in the pelvic drainage area. It’s the pooling of stagnant blood and stretching of pelvic veins that produces pain in pelvic congestion syndrome.
-
How is pelvic congestion syndrome diagnosed?
The key to the correct diagnosis is the women’s pain history.
The symptoms of pelvic congestion syndrome are:
- Deep, dull aching pelvic pain
- Pain worse after upright positions, like standing and sitting
- Pain worse after exercise, like walking, running and weightlifting
- Pain during or after intercourse
- Back and thigh pain
- Varicose veins around the genitals and in the legs
- Pain relief when lying down
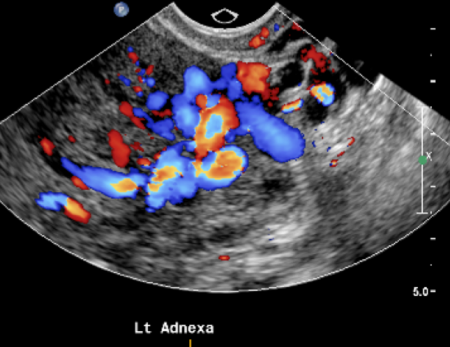
Diagnosis can be made by combining typical symptoms with medical imaging. Pelvic ultrasound quite often detects dilated and congested pelvic varicose veins.
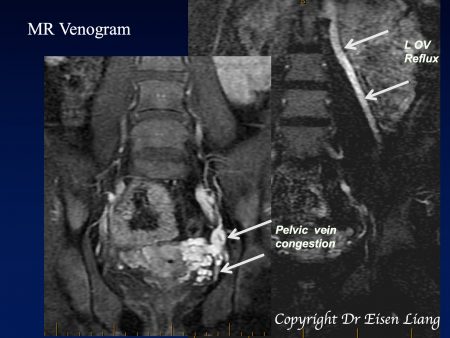
A MRI can not only show congested pelvic veins but also the refluxing ovarian vein – however MRI for this condition is not covered by Medicare.
CT scans can clearly demonstrate pelvic varicose veins as well as the refluxing ovarian vein. The CT scan is most useful for planning the embolisation (blocking) treatment, but involves some radiation and a contrast (X-ray dye) injection.
A dilated pelvic vein can sometimes be discovered incidentally at a laparoscopy when looking for something else. However, laparoscopy is not the appropriate test if one is looking for pelvic congestion syndrome. Pelvic veins are usually collapsed during laparoscopy, due to the head down body tilt and compression by gas used to distend the abdomen.
Pelvic congestion syndrome seems to be an under-recognised and under-diagnosed cause of pelvic pain in women. As chronic pelvic pain can be caused by a variety of conditions, diagnosis of pelvic congestion syndrome is often delayed, as doctors are more inclined to organise tests to rule out more sinister conditions like infection, inflammation and cancer in the bowel and other pelvic organs.
-
How is OVE performed?
Ovarian vein embolisation (OVE) is a local anesthetic procedure performed by an interventional radiologist in an angiography suite, as a day procedure. A light sedation is given, and the skin entry site is numbed with local anaesthetic. Either the jugular or femoral vein is used for entry into the vein.
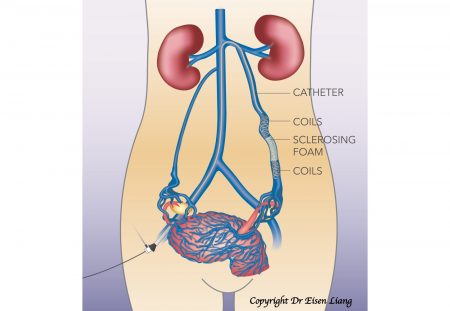
During the process, a tiny nick is made in the skin for a catheter (a small plastic tube) to be inserted. The catheter is navigated inside the vein under X-ray guidance. A venogram is performed by injecting X-ray dye to show the veins and direction of blood flow. Once reflux is confirmed, stainless steel or platinum coils are fed through the catheter to the block the vein. A sclerosing agent is injected to secure long-term blockage of the refluxing veins.
The procedure takes about an hour, but it can be longer if additional refluxing veins are found and need to be treated.
-
How effective is ovarian vein embolisation (OVE)?
OVE is a procedure that blocks the refluxing ovarian vein, targeting the root cause of pelvic congestion syndrome. It is minimally invasive and can be performed as a day procedure under local anaesthetic. Clinical improvement and resolution of symptoms is reported in 83% of patients.
-
What are the advantages of OVE?
Ovarian vein embolisation (OVE) is as effective as laparoscopic ligation, but is much less invasive and less risky. It does not require incisions in the abdomen, therefore allowing for faster recovery and less pain. No general anaesthetic is required and normal activity can be resumed the next day.
-
Is OVE painful?
A small amount of local anaesthetic is injected at the skin to allow the insertion of the catheter into the vein. Ovarian vein embolisation itself is not a painful procedure. In some patients, injection of the sclerosing agent (Fibroivein) can cause pain in the back or the pelvis, that can last for 1 – 2 days after embolisation. This pain can be controlled with Panadol and Nurofen.
-
What are the risks of OVE?
Although uncommon, minor complications such as bruising at the entry site may occur. Vessel injuries and drug allergies are rare, and coil loss in the lungs is extremely rare.
-
Am I a candidate for OVE?
If you’re troubled by the symptoms of pelvic congestion syndrome, ovarian vein embolisation (OVE) could be an ideal pelvic congestion syndrome treatment. For more information on whether you’re a suitable candidate for OVE, ask your GP for a referral and book a consultation with Dr Eisen Liang.
-
How do I recover after OVE?
After OVE, patients require bed rest for 1 – 2 hours until the sedation wears off and will need to arrange transport, as driving is not allowed for 24 hours after sedation. Patients should take it easy at home, drink plenty of fluid and can resume normal activities the following day – though strenuous exercise should be avoided initially. The dressing should be kept for two days and removed afterwards. Some patients may experience back and pelvic pain for 1 – 2 days after embolisation, though this can be controlled with Panadol and Nurofen. Follow-up with Dr Liang is scheduled one month after the procedure.
-
Do I need to see a gynaecologist about OVE?
Sydney Fibroid Clinic believes in a multidisciplinary approach to diagnose and treat pelvic pain. It is important that other potential causes of pelvic pain have been ruled out by your GP and gynaecologist.
By now, you should already have had a pelvic examination, Pap smear, pelvic ultrasound and perhaps other appropriate tests by your GP or gynaecologist. Your GP and gynaecologist will also take part in your follow-up, as well as your ongoing care.
Contact Sydney Fibroid Clinic
If you’re troubled by symptoms of pelvic congestion syndrome and simple measures have not been effective, OVE could be a viable pelvic congestion syndrome treatment for you; especially if you wish to preserve your uterus, avoid major surgery and recover quickly.
If you’re unsure and would like a specialist opinion, ask your GP for a referral and book a consultation with Dr Liang.