By Dr Eisen Liang- fibroid embolisation specialist @ Sydney Fibroid Clinic
- Who needs a hysterectomy?
- How is a hysterectomy done?
- What are the benefits of hysterectomy over other treatment options?
- What are the perceived benefits of keeping your uterus?
- Should hysterectomy be done to prevent cancers?
- What are the risks of hysterectomy?
- What are the long-term side effects of hysterectomy?
- Is hysterectomy still the only solution for heavy painful periods?
If you are looking for alternatives to hysterectomy, check out
UAE for Adenomyosis related heavy painful periods
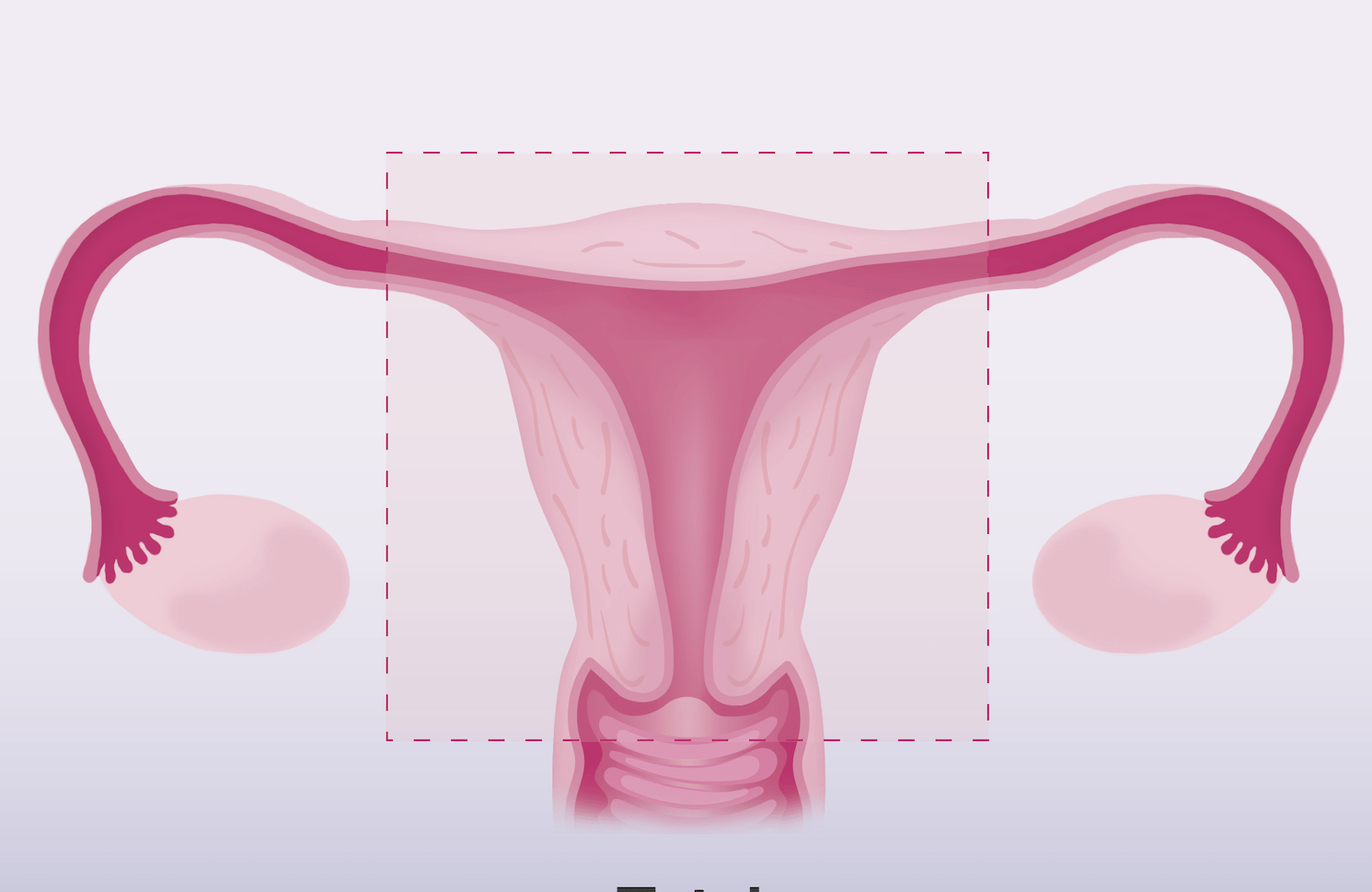
What is a Hysterectomy?
A hysterectomy is a surgical procedure to remove the uterus from a woman. It requires a general anaesthetic, 2-6 days of hospital stay, and 4-6 weeks of recovery.
It’s regarded as a major surgery and therefore carries the risks of a major surgery, such as those associated with general anaesthetics, blood transfusion, wound infection and haematoma, as well as injuries to the bowel, bladder, and ureter (the tube that connects the kidney to the bladder).
What conditions would require a hysterectomy?
If you had cancer of the uterus, you may not have any choice but to have the uterus removed. However, an overwhelming majority of hysterectomies in the developed countries, such as the USA and Australia, are performed for benign conditions such as uterine fibroids and adenomyosis. Since there are now many effective non-surgical means to treat fibroid and adenomyosis, hysterectomy for these benign conditions should be considered as a last resort, when all other less-invasive methods in treating the symptoms have failed.
There are non-surgical treatments as alternative to hysterectomy for fibroids and adenomyosis offfered by Sydney Fibroid Clinic. Find out more:
Fibroid treatment options: https://sydneyfibroidclinic.com.au/fibroids/fibroid-treatment/
Adenomyosis treatment options: https://sydneyfibroidclinic.com.au/adenomyosis/adenomyosis-treatment/
What are the perceived benefits of a hysterectomy?
Hysterectomy has been regarded as the ultimate cure for heavy menstraul bleeding. The uterus, that is the source of heavy menstrual bleeding, is removed, and thereby the symptom of heavy bleeding is eliminated. If the pain is from adenomyosis alone, it will be eliminated as well. Bladder and pressure symptoms will also be relieved instantly. If the cervix is removed, there will be no more Pap smears, and obviously, no further need for contraception. The small risk of developing uterine cancer is also eliminated.
What are the different types of hysterectomies?
There are several types of hysterectomy, depending on the indication for having one.
- Partial (subtotal) hysterectomy: only the body of the uterus is removed, leaving behind the cervix.
- Total hysterectomy without oophorectomy: the entire uterus and cervix are removed, but the ovaries are left behind, Fallopian tubes are usually removed.
- Total hysterectomy and bilateral salpingo-oophorectomy: the entire uterus, including the cervix and fallopian tubes, as well as both ovaries, are removed.
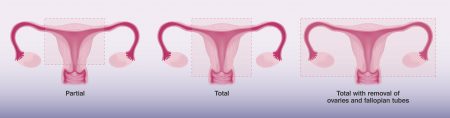
Different types of hysterectomies
What are the different ways of removing the uterus?
There are many ways of removing the uterus, which depend on the woman’s needs, the surgeon’s skill, experience, and preference, and of course, the reason for the hysterectomy.
- Abdominal hysterectomy: performed through a 15cm incision in the lower abdomen. Also called an open hysterectomy.
- Vaginal hysterectomy: performed through a speculum in the vagina (the cervix will have to be removed).
- Laparoscopic hysterectomy: this is the so-called keyhole surgery. Through three or four small cuts in the abdomen, the surgeon inserts a camera and other surgical instruments.
- Laparoscopically assisted vaginal hysterectomy: combines laparoscopic technique with vaginal hysterectomy.
- Laparoscopic or robotic single site hysterectomy: a modified laparoscopic or robotic technique in which the surgeon performs hysterectomy through a single incision.

Different ways to remove the uterus: 0pen abdominal hysterectomy; laparoscopic (keyhole) hysterectomy; robotic single port hysterectomy.
Pros and cons of laparoscopic vs open hysterectomy
Laparoscopic surgery involves 3-4 very small incisions in the lower abdomen. Therefore, the recovery is quicker. However, the surgical risks are not necessarily lower. The cost is often higher, especially if robotic techniques are used. Laparoscopic surgery is technically more demanding, and there’s a steeper learning curve for surgeons.
Due to limited access and visualization, it can be riskier in terms of injuries to blood vessels, bowel, bladder, and ureter. Whether laparoscopic surgery is the right choice for you depends on the reason for your hysterectomy, any other associated problems (like previous surgeries, endometriosis), your desire for a quick recovery, as well as the skill and experience of the surgeon.
Cochrane reviews on hysterectomies (As of October 2020):
These are the main points regarding the review of available evidence by Cochrane:
- Vaginal hysterectomy has a quicker recovery than abdominal hysterectomy.
- Laparoscopic hysterectomy has a quicker recovery than abdominal hysterectomy, but has a greater risk damaging the bladder and ureter and also has a longer operating time.
- There is lack of evidence to suggest robotic hysterectomy is better than laparoscopic hysterectomy.
- Subtotal hysterectomy does not offer improved outcomes for sexual, urinary, or bowel function when compared with total abdominal hysterectomy.
References:
https://www.cochrane.org/CD004993/MENSTR_subtotal-versus-total-hysterectomy
Should ovaries or tubes be removed at the time of hysterectomy for benign diseases?
Some would argue that removing the ovaries at the time of a hysterectomy could potentially reduce the risk of ovarian cancer and the need for future gynaecological procedures. However, premenopausal women who’ve had their ovaries removed also reported an increased risk of cardiovascular disease and other complications due to early menopause.
The evidence provided by observational studies does not support high numbers of prophylactic oophorectomy being done on premenopausal women without BRCA mutations. The lifetime risk of developing ovarian cancer is 1/80, while the lifetime risk of breast cancer is 1/8. If we argue that ovaries should be removed to prevent cancer, then perhaps all women should have their breasts removed to prevent breast cancers. Clearly this is not an acceptable argument for most women and their doctors.
In more recent years, it’s been understood that most ovarian cancers develop from the fallopian tubes. Therefore, the current practice is to remove only the tubes at the time of hysterectomy to prevent ovarian cancer. However, although this makes sense, there are no studies that prove this practice is an effective means of preventing ovarian cancer. Critics of this approach caution against possible injury to the blood supply of the ovaries, which shares their blood supply with the fallopian tubes. This can potentially result in early menopause, even if only the tubes are removed.
Current evidence suggests that routine removal of ovaries during hysterectomy is not generally recommended, while routine removal of the fallopian tubes should be an option that’s discussed with women planning hysterectomy.
References:
Should hysterectomy be performed to prevent uterine cancer?
The lifetime chance of developing a uterine cancer is 1/33. Over 90% of all uterine cancer is endometrial cancer (cancer of the lining of the uterus), which can be detected early. Ultrasound can demonstrate thickening of the lining and the diagnosis is made by endometrial biopsy. The symptoms are bleeding in between periods or after menopause. Risk factors are obesity, type 2 diabetes, and an increased (either longer duration or higher levels of) exposure to oestrogen.
Adenomyosis itself is a benign disease, due to the presence of endometrial tissue in the uterine muscle wall. Questions have been raised regarding whether endometrial cancer can develop within adenomyotic tissue. Studies have shown that this occurs very rarely. Only 3% of endometrial cancers develop from adenomyotic tissue, so therefore the lifetime chance of endometrial cancer developing from adenomyosis is less than 1/1,000. This means it’s a very rare occurrence, and it tends to appear in postmenopausal women with a mean age of 65. On this basis, it doesn’t make sense to perform hysterectomy for adenomyosis to prevent endometrial cancer.
The more problematic uterine cancers to diagnose are those arising from the uterine muscle wall, known as sarcomas, which account for less than 10% of all uterine cancers. Sarcomas are exceedingly difficult to distinguish from fibroids, which are common benign tumours of the uterine muscle wall. The lifetime risk of sarcoma is less than 1/330, and the lifetime risk of a fibroid is more than 1/2 (fibroids can be present in up to 70% of women). Sarcoma is present in only 3/1,000 hysterectomies performed for fibroids.
In other words, sarcomas are rare. Rapid growth and the large size of a uterine tumour does not predict the presence of a sarcoma, and ultrasound can’t reliably diagnose a sarcoma. Advanced MRI (diffusion-weighted imaging DWI) might raise suspicion. Continual growth of a fibroid after menopause in an women not on HRT raises concern.
Fortunately, over 97 % of sarcomas are slowly growing. If a particular uterine fibroid remains viable after embolisation, a hysterectomy may be needed to rule out a sarcoma. It’s important to attend MRI follow-ups after having UAE, to ensure a sarcoma has not been missed. Fear of sarcoma shouldn’t normally be construed as a reason for hysterectomy. The American College of Obstetricians and Gynaecologists does not recommend a hysterectomy solely to rule out sarcoma.
Let’s put things into perspective. The lifetime chance of a women developing breast cancer is 1/8, lung cancer 1/17, colon cancer 1/25, and ovarian cancer 1/80. The lifetime chance of developing a sarcoma of the uterus is less than 1/330, while an endometrial cancer from adenomyosis is less than 1/1,000. If we’re not promoting the notion of removing breasts to prevent breast cancer, it makes no logical sense to remove a woman’s uterus to prevent these rare uterine cancers.
References:
- https://www.cancer.org/cancer/cancer-basics/lifetime-probability-of-developing-or-dying-from-cancer.html
- Correlation between Adenomyosis and Endometrial cancer: 6-year experience of a single centre. Zouzoulas OD, Tsolakidis D, Efstratiou I, Pervana S, Pazarli E, Grimbizis G. Facts Views Vis Obgyn. 2018;10(3):147-152.
Why should women try to avoid hysterectomies?
Hysterectomy is a major surgical operation that requires general anaesthetic, a few days in hospital, and 4-6 weeks of downtime to recover. Hysterectomy is associated with surgical complications and long-term side effects. If you have benign diseases like fibroids and adenomyosis, there are now effective alternative treatments, and therefore hysterectomy should be regarded as a last resort, when less invasive treatments have failed.
What are the hysterectomy risks?
Risks include anaesthetic complications, blood transfusion, DVT, and injuries to other organs.
Since hysterectomy is a major surgery, it’s associated with the risks of any major operation, including those associated with general anaesthetic, blood transfusion, infection, wound healing, and deep venous thrombosis. Rare but severe hysterectomy complications are injuries to the bladder, ureter (the tube connecting the kidney and bladder), bowel, and blood vessels, that might mean a second trip to the theatre with another specialist to repair the damage.
To date, the risk of severe complications from hysterectomy remains at 3.5 to 11.0 %1.
Studies from Melbourne reported a hysterectomy mortality rate of 1.5 /1,000 in Australia2.
Hysterectomy long-term side-effects
- Early menopause
- Prolapse
- Incontinence
- Sexual dysfunction
- Constipation
- Coronary heart disease.
Women who’ve had hysterectomies may enter menopause almost 4 years earlier. The blood supply to the ovaries may be compromised during surgery by ligation, spasm, or thrombosis. Early menopause is known to be associated with increased cardiovascular risk such as heart attacks and strokes, as well as osteoporosis. Premature menopause can also increase the risk of dementia.
A woman’s ovaries continue to produce small, measurable amounts of oestrogen for at least ten years after the start of menopause and to produce androgens until at least age 80. The androgens are converted to oestrogens by fatty tissue and muscle. Oestrogen produced by the ovaries reduce the risk of osteoporosis and heart disease, and it may also help to maintain cognitive and sexual function.
Androgen affects bone and muscle mass, drives libido, affects lipid metabolism, and gives women a sense of well-being, energy, and appetite.
Preservation of the ovarian production of oestrogen and androgen, albeit reduced compared to the reproductive years, may contribute significantly to a woman’s health. This is another rationale for preserving one’s genital organs.
It is well known that hysterectomy may cause prolapse and incontinence many years later. Urologists are familiar with women who complain bitterly of urinary symptoms related to a previous hysterectomy. They’ll say, “Everything was all right, until I had my hysterectomy”.
Hysterectomy weakens the supports for the upper and mid-vagina, and can cause stress urinary incontinence. Removal or cutting of the ligaments supporting the cervix and vagina may predispose women to the development of vaginal vault prolapse. Furthermore, the effectiveness of prolapse repair can be compromised by the removal of the cervix and ligaments, which are used to anchor an effective repair.
Studies regarding the effect of hysterectomy on a woman’s sex life can be confusing. Essentially, it depends on whether her symptoms that led her to consider hysterectomy were affecting her sex life in the first place. Women whose sex life was ruined by menstrual symptoms might find hysterectomy “liberating”, improving the sex life that they didn’t previously have.
On the other hand, women whose sex life was not affected by their menstrual symptoms need to be aware that studies have demonstrated decreased libido and altered orgasm sensation, especially after total hysterectomy. Nerve damage during surgery may be a cause.
For some women, uterine contraction is essential for orgasm. This could be lost after hysterectomy, leading to failure to orgasm or changes in the nature of them.
Surgery may also change the anatomy of the top of the vagina, resulting in an altered sensation for women and their partners.
Constipation following hysterectomy has been reported, and this may be a result of nerve injury.
Woman who’ve had a hysterectomy take longer to recover than those who’ve undergone other major surgeries. Symptoms include urinary problems, tiredness, and depression, and the underlying cause is uncertain. This condition has been labelled Post Hysterectomy Syndrome and is thought to be due to hormone imbalance after hysterectomy.
Registry studies have shown that removing ovaries during a hysterectomy can cause long-term health risks like cardiovascular disease and affect general well-being.
A recent Mayo Clinic study has shown that hysterectomy, even without removal of the ovaries, is associated with a 33% increased risk of coronary heart disease. The risk is increased by 250% if the hysterectomy is performed on women younger than 35 years of age.
Finally, the uterus has a great psychological and cultural significance for some women, whose views and feelings should be respected. For some, removal of their uterus means they might lose their womanhood or sense of being a woman. For those who’ve never been pregnant, keeping their uterus gives them a sense of hope, despite their age and other adverse factors that might affect their chances.
Some women are strongly opposed, in principle, to the removal of any organ, genital or otherwise, unless absolutely necessary. Practitioners should always respect a woman’s view regarding their bodily integrity.
Is hysterectomy still the only solution in the 21st Century?
It’s obvious that in the event of a woman developing a cancer of the uterus, a hysterectomy is a logical and absolute necessity. However, in a developed country like Australia, the majority of hysterectomies are performed for benign conditions like fibroids or adenomyosis.
Is hysterectomy still the only solution in the 21st Century?
Women have the right to question the necessity of a hysterectomy for their mentrual health-related issues. It should be the obligation of the treating doctor to present them with all treatment options available, giving them the pros and cons of each one. They should do so honestly, even if they’re not the providers of some of the options discussed. If a woman elects not to have a hysterectomy, the doctor is obligated to support her in her decision, even when it means a referral to another specialist.
There are non-surgical treatments as alternative to hysterectomy for fibroids and adenomyosis offfered by Sydney Fibroid Clinic. Find out more:
Fibroid treatment options: https://sydneyfibroidclinic.com.au/fibroids/fibroid-treatment/
Adenomyosis treatment options: https://sydneyfibroidclinic.com.au/adenomyosis/adenomyosis-treatment/
Are we doing too many hysterectomies in Australia?
Australia’s national hysterectomy rate is one of the highest amongst OECD countries. We perform 215 per 100,000 women per year, while Demark performs just 20 per 100, 000. Yet there are no major differences between the two countries in terms of longevity, mortality, and quality of life. Similar countries like the UK, Ireland and New Zealand all have about half the hysterectomy rate of Australia. We do about 30,000 hysterectomies each year, and more than 90% are for a benign indication. The question to ask is, “Are they really necessary?”
References
- UpToDate 2019 : Differentiating uterine leiomyomas (fibroids) from uterine sarcomas Elizabeth A Stewart, MD https://www.uptodate.com/contents/uterine-fibroids-leiomyomas-differentiating-fibroids-from-uterine-sarcomas Accessed 28th August 2019
- Ten-year review of hysterectomy morbidity and mortality: can we change direction? Varol, N; Healey, M; Tang, P; Sheehan, P; Maher, P; Hill, D Australian & New Zealand Journal of Obstetrics & Gynaecology, 2001 Aug, Vol.41(3), pp.295-302
- The association of hysterectomy and menopause: a prospective cohort study. Farquhar CM, Sadler L, Harvey SA, Stewart AW. BJOG: An International Journal of Obstetrics & Gynaecology. 2005;112(7):956–962.
- Urinary Symptoms following hysterectomy Smith P, Roberts M, Slade N. British Journal of Urology. 1970;42(1):3–9.
- Supra Vaginal Uterine Amputation VS. Hysterectomy: Effects on libido and orgasm. Kilkku P, Grönroos M, Hirvonen T, Rauramo L. Acta Obstetrica et Gynecologica Scandinavica. 1983;62(2):147–152.
- Papachrysostomou M. Disordered colorectal motility in intractable constipation following hysterectomy. Smith A, Varma J, Binnie N, British journal of surgery. 1990;77(12):1361–1365.
- A post-hysterectomy syndrome. Richards D. The Lancet. 1974;304(7887):983–985.
- Cardiovascular and metabolic morbidity after hysterectomy with ovarian conservation: a cohort study Laughlin-Tommaso, K., Shannon; Khan, L., Zaraq; Weaver, Y., Amy ; Smith, A., Carin ; Rocca, A., Walter ; Stewart, A., Elizabeth Menopause, 2018, Vol.25(5), p.483-492
- OECD Hysterectomy Rate: https://stats.oecd.org/
