In A Nutshell
- Mirena is a progestogen-releasing contraceptive IUD.
- Mirena alleviates adenomyosis-related HMB and pain in a majority of women.
- Common side effects are irregular bleeding and spotting.
- Mirena might not work well for a uterus larger than 150ml.
Failing Mirena , check out UAE as an non-surgical alternative to hysteretomy
Mirena for Adenomyosis
Mirena, a hormone-releasing IUD, is commonly used for heavy menstrual bleeding and period pain. A significant majority of women have a positive experience with it in terms of its effectiveness and lack of side effects. Apart from UAE, Mirena is currently the best-evaluated and the most efficacious non-surgical treatment for adenomyosis-related heavy bleeding and period pain.
Mirena is also an effective contraceptive device that might be appropriate for some women, as once removed, they can try to get pregnant straight away. It’s also useful in treating period pain associated with endometriosis, which often coexists with adenomyosis.
Many women might stop having a period altogether. This happens in up to 8% of women at 6 months, and 16.8% at 12 months. This is desirable for some women but might not be for others.
As with all medical therapies, Mirena isn’t effective for everyone, and some women do develop significant side effects. In our specialist tertiary referral clinic, we tend to see women who’ve found that Mirena didn’t help them or were trying to avoid having it.
Its failure could be simply ineffectiveness. For these women, their menstrual bleeding was still heavy and/or painful. In some, their bleeding had been so heavy, that the Mirena was expelled. For others, it might have worked for some time, but as the disease progressed, it stopped working.
One of the common issues with Mirena is that it might take 3 to 6 months to “settle in” and become effective. During that time, there could be irregular bleeding, continuous light bleeding, or spotting. Women are often encouraged to persevere for that length of time, with the expectation that it might eventually work. Many women follow this advice but then become rather fed up with having to wear a pad every day for so many months. They get frustrated and just want it out. What follows is that, unless there are other backup therapies in place, they might suffer from a severe withdrawal bleed with flooding and clotting, once their Mirena is removed.
Some women are unlikely to have a good response with Mirena. Sadly, we didn’t know about this until recently. A 2016 study from Korea has shown Mirena is less effective in women with more extensive adenomyosis. They found that if a woman’s uterus was larger than 150ml, Mirena was more likely to be discontinued. And in women whose uterus was larger than 314ml in volume, the rate of discontiuation was 70%.
When the uterine cavity is distorted due to fibroids or focal adenomyosis, Mirena might not sit well, be difficult and risky to insert, and is more likely to be expelled.
Some women come to see us looking for alternatives. Others have experienced side effects like weight gain, mood swings, bloating, and abdominal pain. Many are concerned about having it inserted after reading about these side effects online or hearing about them from their friends.
Mirena insertion can be uncomfortable for women who haven’t had a vaginal birth, because the cervical canal can be rather tight, so it might have to be done under sedation with local anaesthetic gel.
If your Mirena is not effective or if you are developiong side effects, UAE (uterine artery embolisation) is effective in alleviating heavy menstrual bleeding and period pain. UAE is a non-hormonal and non-surgical treatment, and can be used as an alternative to hysterectomy.
More about Mirena and adenomyosis
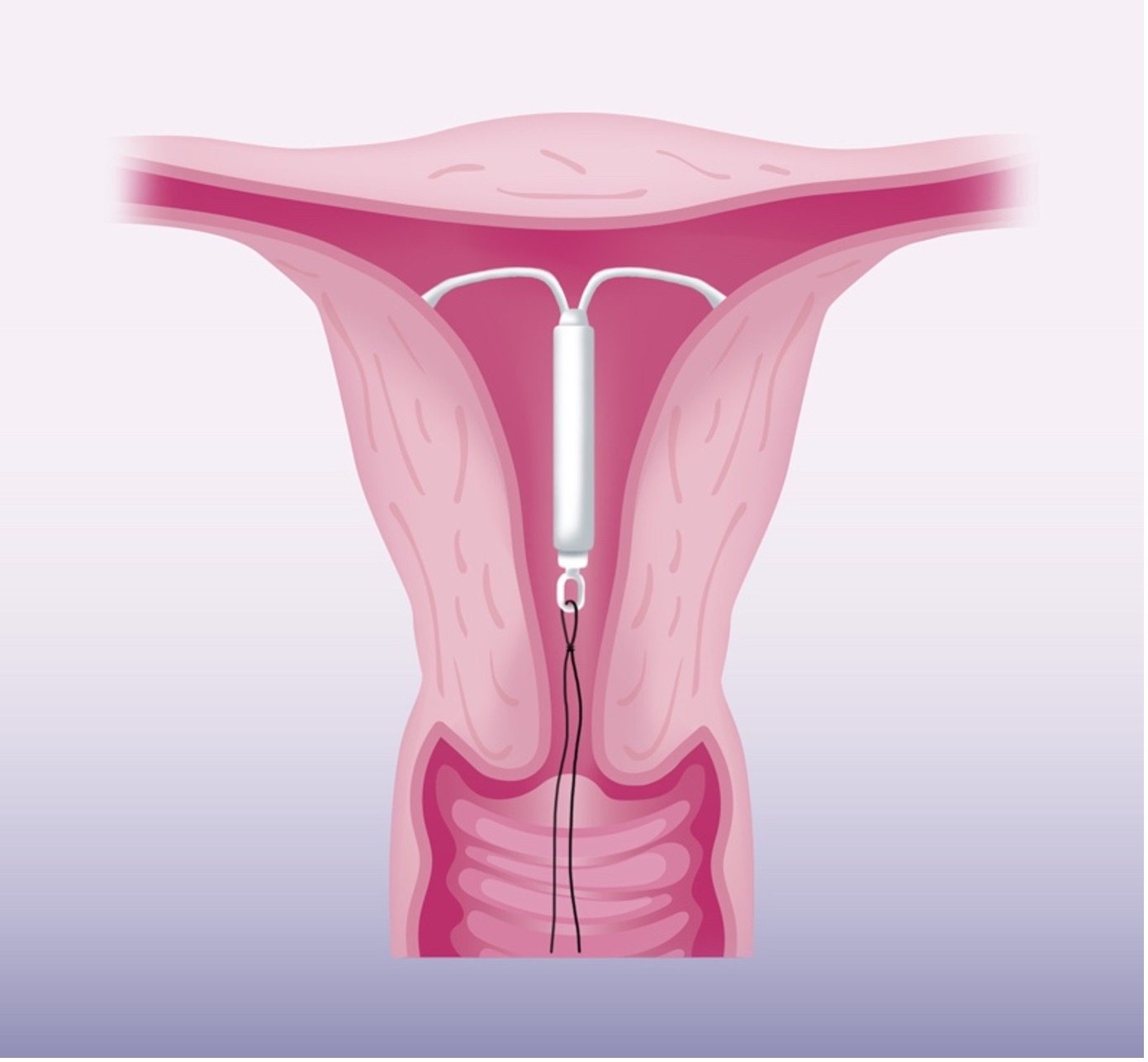
Mirena is an intrauterine device that slowly releases a tiny dose of progestogen over 5 years. It was initially designed as a contraceptive device, but it has been commonly used for control of heavy menstrual bleeding.
It’s T-shaped, with two soft plastic flexible arms measuring 3.2 cm total width across. The tubular body, 3.2 cm in height, houses the progestogen reservoir. The device can be inserted in a doctor’s office, or if insertion difficulty is expected, it can be done under ultrasound guidance with sedation.
We don’t completely understand how it reduces heavy menstrual bleeding, but it has been hypothesised to work in two ways. First, the slowly released progestogen causes thinning of the endometrial lining and therefore decreases the amount of menstrual flow. Second, the high local concentration of progestogen turns down the responsiveness of oestrogen receptors in the adenomyotic tissues and prevents oestrogen stimulation of the adenomyotic foci, causing them to shrink. This allows better uterine muscle contraction to help reduce menstrual blood loss.
A study from the Women’s Health Teaching and Research Hospital in Turkey confirmed the effectiveness of Mirena in reducing menstrual blood flow. The study compared Mirena with abdominal hysterectomy. It was published in 2011 in the journal “Fertility and Sterility” and showed a similar outcome in controlling heavy menstrual bleeding. This was a randomised control study, with 43 women assigned to Mirena and 43 assigned to hysterectomy. The haemoglobin level of the women in the study was measured at 6 and 12 months. Both groups showed comparable increase in haemoglobin by 20 grams/L. At 6 months, with 23.8% of women reporting having no period bleeding, while at 12 months, 51.4% reported no more period bleeding.
The side effects reported were headache (11.9%), breast tenderness (7.1%), acne (4.8%), and transient depression (2.4%). Health-related quality of life was measured and showed improvement in both groups. Mirena was superior to hysterectomy on improvement in psychological and social life. The study concluded that Mirena may be a promising alternative to hysterectomy.
A 3-year follow-up study from Beijing O&G Hospital in China, showed Mirena was also effective in reducing period pain. The study followed 94 women with adenomyosis treated with Mirena. A significant drop in menstrual pain score was noted, from 77.9 at baseline, to 16 at 12 months and 11.8 at 36 months. However, the patient satisfaction rate was only 56.3% at 12 months. The common side effects reported were prolonged light bleeding (25%) or irregular bleeding (14%). Other less-common side effects were weight gain (28.7%), ovarian cyst formation (22.3%), lower abdominal pain (12.8%), acne (6.4%), and transient depression (1.1%). These side effects might have contributed to the less-than-ideal satisfaction rate. At one year, 12% of Mirena had been expelled, and10.6% were removed due to side effects, resulting in a 22.6% discontinuation rate.
Possible Mirena Side Effects
(List from Bayer Consumer Medicine Information)
- Nervousness, depressed mood, mood swings
- Lower abdominal/pelvic pain or back pain, period pain
- Bleeding changes, including:
- increased or decreased menstrual bleeding,
- spotting, infrequent or light periods,
- absence of bleeding
- Headache, migraine, nausea
- Acne, excessive hairiness
- Tender or painful breasts
- Itching, redness, and/or swelling of the vagina, vaginal discharge
- Weight gain
- Decreased libido
- Expulsion of Mirena
If you are not tolerating these side-effects, consider UAE as a non-hormonal treatment, effective in 90% of women with heavy and painful periods. Learn more about UAE.
References
- Mirena Consumer Medicine Information
https://www.ebs.tga.gov.au/ebs/picmi/picmirepository.nsf/pdf?OpenAgent&id=CP-2010-CMI-03485-3&d=202010031016933 - FDA Data
https://www.accessdata.fda.gov/drugsatfda_docs/label/2008/021225s019lbl.pdf - Levonorgestrel intrauterine system associated amenorrhea: a systematic review and metanalysis, Jill E. Sergison, Lauren Y. Maldonado, Xiaoming Gao, David Hubacher, AJOG Systemic Reviews| Vol 220, Issue 5, P440-448.E8, MAY 01, 2019
- An update on the pharmacological management of adenomyosis. Streuli I, Dubuisson J, Santulli P et al. Expert Opinion on Pharmacotherapy, 11/2014, Volume15, Issue 16
- Adenomyosis: A Clinical Review of a Challenging Gynecologic Condition. Struble, Jennifer; Reid, Shannon; Bedaiwy, Mohamed A. Journal of Minimally Invasive Gynecology. 2016 23 (2): 164185.
- Comparison of levonorgestrel intrauterine system versus hysterectomy on efficacy and quality of life in patients with adenomyosis. Ozdegirmenci O, Kayikcioglu F, Akgul MA, et al. Fertil Steril 2011;95(2):497-502
- The LNG-IUS study on adenomyosis: a 3-year follow-up study on the efficacy and side effects of the use of levonorgestrel intrauterine system for the treatment of dysmenorrhea associated with adenomyosis. Sheng, J, Zhang, J P, Zhang, W Y et al. Contraception, 2009, Volume 79, Issue 3
- Relationship between uterine volume and discontinuation of treatment with levonorgestrel-releasing intrauterine devices in patients with adenomyosis. Lee, Ki Hwan; Kim, Jang Kew; Lee, Min A; Ko, Young Bok; Yang, Jung Bo; Kang, Byung Hun; Yoo, Heon Jong Archives of Gynecology and Obstetrics, 2016, Vol.294(3), p.561(6)
